Benemid (Probenecid) vs Alternatives: A Practical Comparison
 Oct, 9 2025
Oct, 9 2025
Benemid vs Alternatives: Drug Comparison Tool
Drug Comparison Details
Quick Summary
If you’ve ever been told to lower your uric acid, you probably heard the name Benemid. But you might wonder whether it really beats the other drugs on the market or if another option fits your lifestyle better. Below we break down how Benemid works, who benefits most, and how it stacks up against the most common alternatives.
What is Benemid (Probenecid) and How Does It Work?
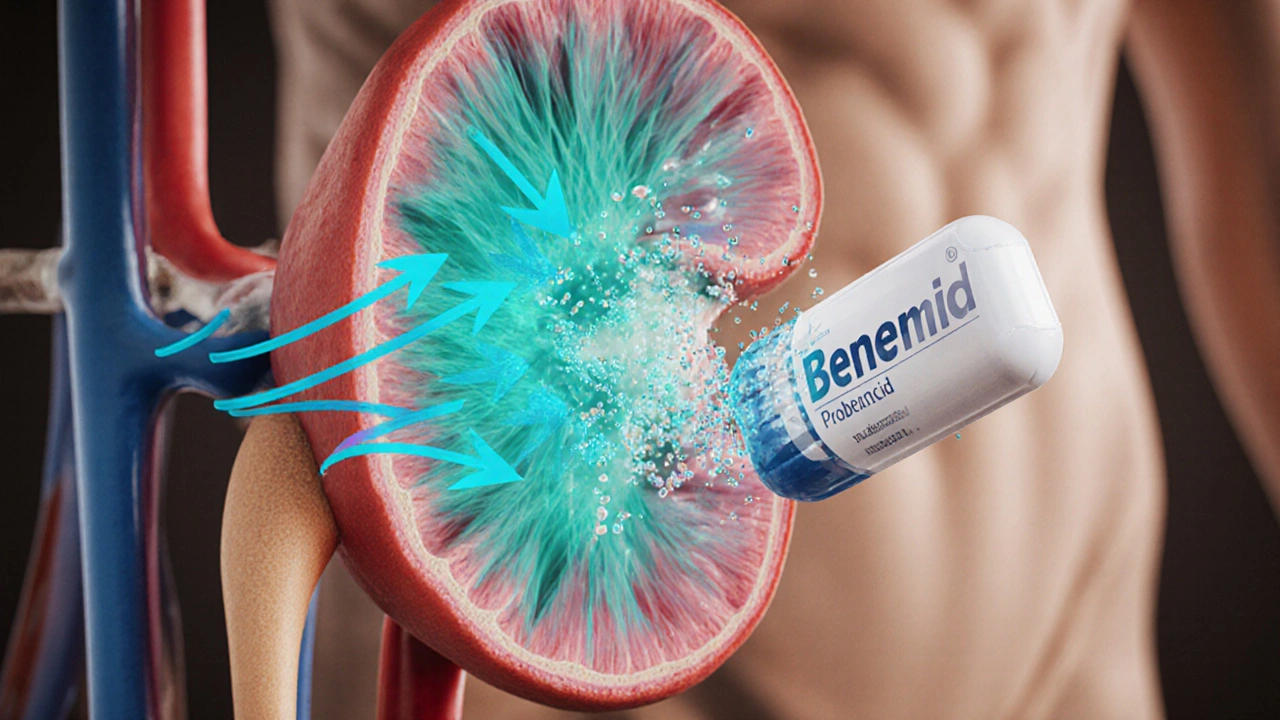
Benemid is a uricosuric agent that increases the renal excretion of uric acid by inhibiting its reabsorption in the proximal tubules. By keeping more uric acid in the urine, it lowers blood levels and reduces the risk of gout flares.
In contrast to xanthine oxidase inhibitors, which block uric acid production, Benemid tackles the problem from the elimination side. The drug works best when kidney function is relatively preserved, because it relies on active tubular transport.
Key Alternatives on the Market
Most patients with gout eventually try one of these agents:
- Allopurinol is a xanthine oxidase inhibitor that reduces uric acid synthesis.
- Febuxostat is a newer, non‑purine xanthine oxidase inhibitor offering a once‑daily dose.
- Lesinurad is a selective uric‑acid transporter 1 (URAT1) inhibitor used in combination with a xanthine oxidase blocker.
- Pegloticase is an intravenous uricase enzyme that enzymatically degrades uric acid.
- Colchicine is not a urate‑lowering drug but a fast‑acting anti‑inflammatory used for acute flares.
Each option has its own profile of efficacy, safety, dosing convenience, and cost.
When Does Benemid Shine?
Benemid is most useful in three scenarios:
- Patients who cannot tolerate allopurinol or febuxostat due to hypersensitivity or severe skin reactions.
- People with underexcreted uric acid (low urinary uric acid excretion) where a uricosuric approach resolves the underlying issue.
- Patients already on low‑dose allopurinol who need an extra uric‑lowering push without increasing the allopurinol dose.
Because Benemid increases uric acid levels in the urine, it can raise the risk of kidney stones. Adequate hydration (aim for >2L/day) and regular urine pH monitoring are essential to mitigate that risk.

Comparing Efficacy and Safety
Head‑to‑head studies show that when used at the standard 500mg bid dose, Benemid lowers serum uric acid by about 25‑30%. Allopurinol typically achieves a 30‑35% reduction, while febuxostat can reach 35‑40% in patients with normal renal function. Lesinurad adds roughly 15‑20% when paired with a xanthine oxidase inhibitor. Pegloticase, reserved for refractory cases, can drop uric acid to near‑zero within days.
Safety-wise, Benemid’s most common side effects are mild gastrointestinal upset and the aforementioned stone formation. Allopurinol’s concerns center on rash and, rarely, Stevens‑Johnson syndrome. Febuxostat carries a boxed warning for cardiovascular events, especially in patients with existing heart disease. Lesinurad may cause renal impairment if combined with high‑dose allopurinol. Pegloticase can trigger infusion reactions and requires pre‑screening for anti‑uricase antibodies.
Drug Interactions You Need to Watch
Benemid is a classic inhibitor of renal tubular secretion. This means it can boost blood concentrations of several drugs that use the same transport pathways, such as:
- Penicillins and cephalosporins - risk of toxicity.
- Non‑steroidal anti‑inflammatory drugs (NSAIDs) - may reduce Benemid’s uricosuric effect.
- AZT (zidovudine) - increased hematologic toxicity.
When you’re on a regimen that includes these meds, your doctor might lower the Benemid dose or pick a different urate‑lowering agent.
Choosing the Right Agent: A Quick Decision Guide
| Drug | Mechanism | Typical Dose | Uric‑Acid Reduction | Renal Considerations | Cost (US$/month) |
|---|---|---|---|---|---|
| Benemid (Probenecid) | Uricosuric - blocks reabsorption | 500mg bid | ≈25‑30% | Requires good renal function; risk of stones | ≈30‑40 |
| Allopurinol | Xanthine oxidase inhibitor | 100‑300mg daily | ≈30‑35% | Safe down to eGFR≈30ml/min | ≈15‑20 |
| Febuxostat | Selective xanthine oxidase inhibitor | 40‑80mg daily | ≈35‑40% | Safe to eGFR≈30ml/min; watch CV risk | ≈200‑250 |
| Lesinurad | URAT1 inhibitor (add‑on) | 200mg daily + XO inhibitor | ≈15‑20% (add‑on) | Can worsen renal function if mis‑dosed | ≈150‑180 |
| Pegloticase | Recombinant uricase enzyme | 8U IV bi‑weekly | >90% (rapid) | Not recommended with severe renal disease | ≈1200‑1500 |
Use this table as a snapshot when you talk to your clinician. If you have normal kidney function, are motivated to stay well‑hydrated, and want an oral option that isn’t a production blocker, Benemid may be the sweet spot.
Practical Tips for Getting the Most Out of Benemid
- Take the dose after meals to improve absorption.
- Drink at least 2L of water daily; consider citrate‑based drinks to keep urine pH >6.5.
- Schedule a 24‑hour urine uric acid test after 2weeks to confirm it’s working.
- If you develop flank pain or see blood in urine, stop the drug and get imaging for stones.
- Ask your doctor about a low‑dose aspirin regimen if you need cardiovascular protection-high‑dose aspirin can blunt Benemid’s effect.
Bottom Line
Benemid fills a niche that many other gout meds don’t: it helps people who excrete too little uric acid or can’t tolerate the classic production blockers. Its oral, twice‑daily schedule is convenient, but you must stay on top of hydration and monitor for kidney‑stone symptoms. When evaluating alternatives, weigh efficacy, renal safety, cost, and any existing comorbidities. Talk to your healthcare provider about whether a uricosuric, a production inhibitor, or a combination best matches your health goals.
Frequently Asked Questions
Can I use Benemid if I have kidney disease?
Benemid requires at least moderate kidney function (eGFR>30ml/min). In severe CKD the drug’s ability to push uric acid into the urine wanes, and the stone risk rises, so doctors usually choose allopurinol or febuxostat instead.
How fast does Benemid lower serum uric acid?
Most patients see a 10‑15% drop within the first week, reaching the full 25‑30% reduction after about 4‑6weeks of consistent dosing.
Do I need to stop other gout meds when I start Benemid?
Not necessarily. Benemid is often added to a low‑dose allopurinol regimen when the latter alone isn’t enough. However, you should avoid using two uricosurics together (e.g., Benemid plus lesinurad) because the stone risk skyrockets.
What dietary habits help Benemid work better?
Focus on a low‑purine diet (cut back on organ meats, anchovies, and beer), stay well‑hydrated, and consider alkalinizing agents like potassium citrate if you’re prone to acidic urine.
Is Benemid covered by insurance?
Most U.S. insurers list Benemid on their formulary, but coverage varies by plan. Generic probenecid is cheaper than the brand name and is usually preferred for cost‑savings.
kathy v
October 9, 2025 AT 19:46Benemid, the so‑called “American miracle” for gout, is touted by some as the perfect oral solution, yet its limitations are glaringly obvious to anyone with even a modicum of medical insight.
The drug’s reliance on robust renal function makes it inherently unsuitable for a large swath of our population that suffers from chronic kidney disease, a condition that is especially prevalent in the United States.
Moreover, the risk of kidney stone formation under Benemid is not a trivial inconvenience but a serious health hazard that can lead to emergency interventions and costly procedures.
While proponents point to its low cost, the real expense emerges when patients are forced to purchase alkalinizing agents, extra water, and frequent imaging studies to monitor stone formation.
Allopurinol, by contrast, remains effective even when eGFR falls below thirty, and its safety profile has been vetted over decades of widespread use across the nation.
Febuxostat might be pricier, but its once‑daily dosing and independence from high renal clearance make it a far more reliable option for the average American dealing with comorbidities.
The selective marketing of Benemid as the “go‑to” uricosuric betrays a commercial agenda that disregards the nuanced needs of diverse patient groups.
In a country that prides itself on cutting‑edge healthcare, clinging to a drug that demands perfect hydration and vigilant stone surveillance is frankly antiquated.
Patients who cannot tolerate allopurinol or febuxostat for fear of hypersensitivity should be evaluated for newer therapies rather than being forced back onto an old‑fashioned uricosuric.
The interaction profile of Benemid, especially its inhibition of penicillin excretion, creates a cascade of drug‑drug complications that our healthcare system can ill afford.
There is also the myth that Benemid can be safely combined with any xanthine oxidase inhibitor; such combinations dramatically increase the risk of renal decline and should be avoided.
When the FDA label itself warns about stone risk and the need for diligent monitoring, it is a clear indication that the drug is far from a universal solution.
The American gout patient, often juggling hypertension, diabetes, and cardiovascular disease, needs a therapy that simplifies their regimen, not one that adds layers of complexity.
From a public‑health perspective, encouraging the use of a drug that demands high fluid intake and regular urine pH checks is a recipe for non‑adherence.
Therefore, clinicians must weigh the modest cost savings of Benemid against the substantial burdens it places on patients, insurers, and the broader healthcare infrastructure.
In short, Benemid may have its niche, but to proclaim it the superior choice for the average American is an overstatement that borders on reckless advocacy.
Jorge Hernandez
October 10, 2025 AT 20:46Great breakdown 🙌 Benemid can work if you stay hydrated 💧 and keep an eye on stones 👍
Raina Purnama
October 11, 2025 AT 21:46Thank you for the comprehensive overview. It’s helpful to see the comparison of efficacy, safety, and cost side by side. For patients with adequate kidney function, Benemid offers a convenient oral option, while those with CKD may benefit more from allopurinol or febuxostat. Monitoring urine pH and ensuring sufficient fluid intake remain essential regardless of the chosen therapy.
April Yslava
October 12, 2025 AT 22:46Everyone talks about hydration like it’s a simple fix, but the pharma giants deliberately hide the fact that Benemid’s stone risk is part of a larger scheme to sell more “water enhancers” and “alkaline supplements.” They want us to think it’s our responsibility, not theirs, to stay on top of urine pH. The truth is buried under layers of marketing fluff, and only those who question the narrative see the real danger.
Daryl Foran
October 13, 2025 AT 23:46Honestly the whole Benemid hype is overrated, its effectiveness is meh and side‑effects are undervalued. If you can’t handle a few stones you should just switch to allopurinol.
Rebecca Bissett
October 15, 2025 AT 00:46Oh dear, another comment downplaying a therapy that actually helps many! I feel so frustrated when people ignore the nuanced benefits, especially when patients have limited choices! The emotional toll on those who battle gout daily is immense, and we need compassion, not dismissive remarks!!!
Michael Dion
October 16, 2025 AT 01:46Benemid is cheap.
Trina Smith
October 17, 2025 AT 02:46While cost matters, the true value of a medication lies in its alignment with the patient’s lifestyle and overall health goals 🌱. A low‑price drug that demands rigorous hydration may not be the most practical choice for everyone.
josh Furley
October 18, 2025 AT 03:46Benemid’s pharmacodynamics are suboptimal; the uricosuric pathway is limited by transporter saturation 🚫. Choose a XO inhibitor for consistent urate reduction.
Jacob Smith
October 19, 2025 AT 04:46Yo, i get it bro! Allopurinol is solid, but give Benemid a shot if u stay super hydrated. Keep it up!
Chris Atchot
October 20, 2025 AT 05:46Excellent discussion! It is imperative, however, to emphasize that adherence to any urate‑lowering therapy requires diligent monitoring of renal function, serum uric acid levels, and potential drug interactions. Moreover, patient education regarding dietary purine intake, fluid consumption, and possible adverse effects should be comprehensive and individualized.
Shanmugapriya Viswanathan
October 21, 2025 AT 06:46Honestly, our healthcare system could learn a thing or two from countries that prioritize cost‑effective oral agents like Benemid. 🇺🇸
Rhonda Ackley
October 22, 2025 AT 07:46The moment I read about Benemid, I was swept into a whirlwind of hopes and doubts, like a drama unfolding on a stage of endless medical charts. I imagined myself juggling bottles of water, fearing the dreaded stone that could erupt at any moment, while the pharmacy clerk whispered about the “affordable miracle” that might save my wallet. Yet, each sentence in the drug’s monograph felt like a plot twist-renal requirements here, interaction warnings there-leaving me breathless and yearning for clarity. My mind raced through scenarios where I could either embrace the convenience of a twice‑daily pill or succumb to the tyranny of relentless monitoring. The cost comparison chart, with its glaring $30‑40 versus $200‑250, sparked a theatrical clash between frugality and efficacy. I found myself chanting, “Do I dare to trust the cheap hero, or do I bow to the pricey champion?” In the end, the drama taught me that every medication writes its own story, and the audience-us-must decide which narrative we are willing to follow.
Sönke Peters
October 23, 2025 AT 08:46Both viewpoints highlight valid concerns; patients should weigh cost, efficacy, and safety to choose the best fit.
Paul Koumah
October 24, 2025 AT 09:46Sure, just pop a pill and wait for the magic to happen.
Erica Dello
October 25, 2025 AT 10:46Honestly this attitude is unacceptable 🙄 medication decisions deserve seriousness not sarcasm